Medicare for All or State Control: Health Care Plans Go to Extremes
September 14, 2017 by admin
Filed under Choosing Lingerie
“Instead of wasting hundreds of billions of dollars trying to administer an enormously complicated system of hundreds of separate insurance plans, there would be one insurance plan for the American people with one single payer,” said Mr. Sanders, the ringmaster of an event that felt like a political rally, with banners and placards, consumers and patients, labor union members, nurses in red T-shirts and an audience full of fans who applauded, whooped and hollered.
Heading in the other direction were several Republican senators, led by Lindsey Graham of South Carolina and Bill Cassidy of Louisiana, who would take money spent under the Affordable Care Act and give it to states in the form of block grants.
Their proposal was the last gasp of Republican efforts to undo the Affordable Care Act. Those efforts, which seemed sure of success in January, appeared to meet a dead end on the Senate floor in late July, when Republicans could not muster even a simple majority for a repeal bill. Mr. Graham’s gathering had the feel of a health policy discussion at a conservative think tank.
While Mr. Sanders was joined by possible presidential contenders, Mr. Graham and Mr. Cassidy were accompanied by two lower-profile senators, Dean Heller of Nevada and Ron Johnson of Wisconsin.
Graphic
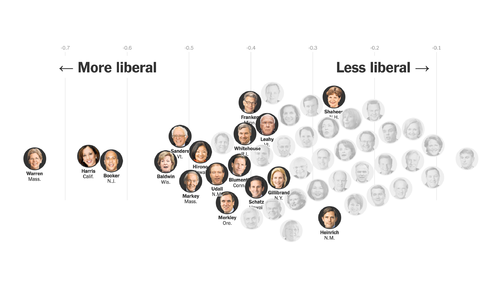
One-Third of Democratic Senators Support Bernie Sanders’s Single-Payer Plan
The ideological makeup of senators who support the health plan.
“The only thing stopping us from having this idea debated on the floor of the United States Senate is lack of leadership,” Mr. Graham said, pleading for help from President Trump and the Senate majority leader, Mitch McConnell of Kentucky.
An hour later Mr. Trump issued a statement saying, “I sincerely hope that Senators Graham and Cassidy have found a way to address the Obamacare crisis.’’
Under the Graham-Cassidy proposal, money would be distributed to states based on a complex formula. The regional cost of living would be one factor, but the sponsors acknowledged that higher-spending states like Massachusetts would receive less than under current law.
Advertisement
Continue reading the main story
The block grant would replace federal money now being spent under the Affordable Care Act for the expansion of Medicaid, for premium tax credits and for subsidies that reimburse insurers for reducing out-of-pocket costs for low-income people.
The Graham-Cassidy bill would repeal the Affordable Care Act’s requirements for most Americans to have coverage and for larger employers to offer it. And it would make deep cuts in Medicaid.
But time is running out on the bill. After Sept. 30, the Graham-Cassidy legislation would lose procedural protections that allow passage in the Senate with a simple majority, rather than the 60 votes often required for major legislation.
Newsletter Sign Up
Continue reading the main story
Thank you for subscribing.
An error has occurred. Please try again later.
You are already subscribed to this email.
Even with those protections, Senator John Cornyn of Texas, the No. 2 Senate Republican, said he had seen no evidence that the bill had the votes needed to win approval in the Senate in the next two weeks. And he noted that it had not been analyzed by the Congressional Budget Office, which could take a week or two to estimate how much the bill would cost and how many people would lose or gain coverage.
Mr. Sanders said he was prepared for a long battle to establish health care as a right. (That was supposedly a goal of the Affordable Care Act.) His bill could serve as a political manifesto and a possible campaign platform for progressive candidates.
That so many Democrats are embracing it is a milestone. About 60 percent of House Democrats have endorsed a “Medicare for all” bill introduced by Representative John Conyers Jr., Democrat of Michigan.

Credit
Tom Brenner/The New York Times
But Democratic leaders in the House and the Senate are steering clear, saying their immediate concern is to protect coverage under the Affordable Care Act, which still faces attacks from Republicans.
Mr. Sanders’s bill would expand Medicare, one of the nation’s largest, most popular entitlement programs. The federal government would establish an annual budget for covered health care services. Medicare’s benefit package would be expanded to include coverage of dental care, vision services and hearing aids. The bill would also cover “comprehensive reproductive, maternity and newborn care, including abortion,” according to a summary prepared by Mr. Sanders’s office.
The federal government would establish a standard list of covered drugs, and the secretary of health and human services would negotiate prices with drug companies.
Advertisement
Continue reading the main story
Mr. Sanders did not say how he would pay for his bill. He issued a list of a dozen financing options, which included higher tax rates for high-income people and “an annual 1 percent federal wealth tax on the net worth of the wealthiest one-tenth of 1 percent of U.S. households.’’
The Sanders bill would eliminate deductibles and most other out-of-pocket costs for consumers, but the government “may impose limited co-payments for prescription drugs in order to encourage the use of lower-cost generic drugs.”
Under the bill, Medicare — now available to people 65 and older and to some younger people with disabilities — would be expanded over four years. In the first year, Medicare would be opened to children through age 18 and to adults from 55 to 64. The eligibility age would be reduced to 45 in the second year and to 35 in the third year, with “every resident of the United States” entitled to benefits in the fourth year.
That would bring huge changes to the health care system, affecting many people who are content with the coverage they have. More than 150 million people under the age of 65 have employment-based coverage. The Sanders bill would separate health insurance from employment, shrinking the role of employers and insurance companies.
Employer-sponsored plans could not duplicate benefits provided by Medicare, but could offer extra benefits.
Mr. Sanders predicted that “insurance companies, drug companies and Wall Street won’t like this legislation,” and he was right.
David Merritt, an executive vice president of America’s Health Insurance Plans, a lobby for insurers, said: “Whether it’s called single-payer or Medicare for all, government-controlled health care cannot work. It will eliminate choice, undermine quality, put a chill on medical innovation and place an even heavier burden on hard-working taxpayers.”
Continue reading the main story